


INTRODUCTION
Delirium is a syndrome characterized by an acute onset of symptoms, such as changes in cognition, altered consciousness, and impaired attention [1]. Three types of delirium are hyperactive (agitated and over aroused), hypoactive (appearing drowsy or depressed) and the mixed type [2]. Delirium is an important clinical problem in nursing homes [3]. In particular, delirium is frequent in the first weeks after admission to nursing homes [4]. The incidence of delirium in nursing homes was reported as ranging from 3.4% to 70.3%, which is a high incidence [5,6]. The wide range of incidence rates can be explained by different study designs, different tools to measure delirium, and differences in populations. Nursing home residents with delirium are more likely to be sent to the emergency department, have a poor functional recovery, and have higher morbidity and mortality [7]. In addition to preventing these consequences, the identification of delirium is important because this condition is potentially reversible, if found early [3]. Nursing home nurses have an important role, providing clinical expertise, logical care management, and the planning of scientific care, based on the timely assessment of residents’ health status [8]. Risk-factor identification of delirium is an important step because it will help nursing home nurses detect residents at high risk for delirium and design and target preventive intervention strategies [9].
Because of the importance of early detection and prevention of delirium, a delirium guideline for elders has been developed. However, all these guidelines are used in settings (i.e., intensive care unit or a general medical/ surgical unit) other than nursing homes [10]. Therefore, an urgent need exists for the development of an evidence-based treatment or guidance on preventive action for delirium in the nursing home. For such guidelines to be developed, identifying risk factors for nursing home residents should be a priority. For the nursing home population, a wider variety of risk factors and conditions can influence delirium than in other setting populations because nursing home residents tend to be older, often have dementia, have physical restraints, and have a higher prevalence of comorbidities [11].
To date, researchers have conducted only systematic reviews of delirium risk factors primarily in intensive care units [12] and with perioperative or postoperative patients [1]. Although the National Government Clearinghouse, National Institute for Health and Care Excellence, and Hartford Institute for Geriatric Nursing have provided delirium guidelines and protocols, these guidelines and protocols are limited to evidence on hospitalized medical surgical patients. Therefore, it is necessary to provide a systematic review of the risk factors of nursing home residents because they have different characteristics than those in acute settings. In particular, in that the main content of delirium-prevention programs is managing risk factors, identifying risk factors is also important. Only fragmentary studies describe the risk factors of delirium in nursing homes, but no study has systematically investigated their results. Therefore, the aim of this systematic review was to explore the reported risk factors for the development of delirium in the nursing home.
METHODS
Systematic review of primary research was undertaken. The approach was based on the systematic-review methods recommended for questions of effectiveness [13].
1. Search Strategy and Data Sources
Four electronic databases were used: CINAHL, Pub Med, EBSCOhost, and Medline. The title, abstract, and keywords were searched to identify relevant journals in July of 2019. Medical Subject Headings (MeSH) terms such as “Delirium” [MeSH], “Nursing home” [MeSH] OR “Long term care facility” [MeSH] AND “Risk factor” [MeSH] were used to retrieve relevant journals. Reference lists of included studies were reviewed to search for relevant studies. The year of publication was not limited.
2. Inclusion Criteria
Inclusion criteria were as follows: (a) primary research, (b) the outcome was the incidence or onset of delirium, (c) articles were written in English with the full text available, (d) peer-reviewed, and (e) multivariable analyses were undertaken to identify factors affecting delirium.
3. Screening
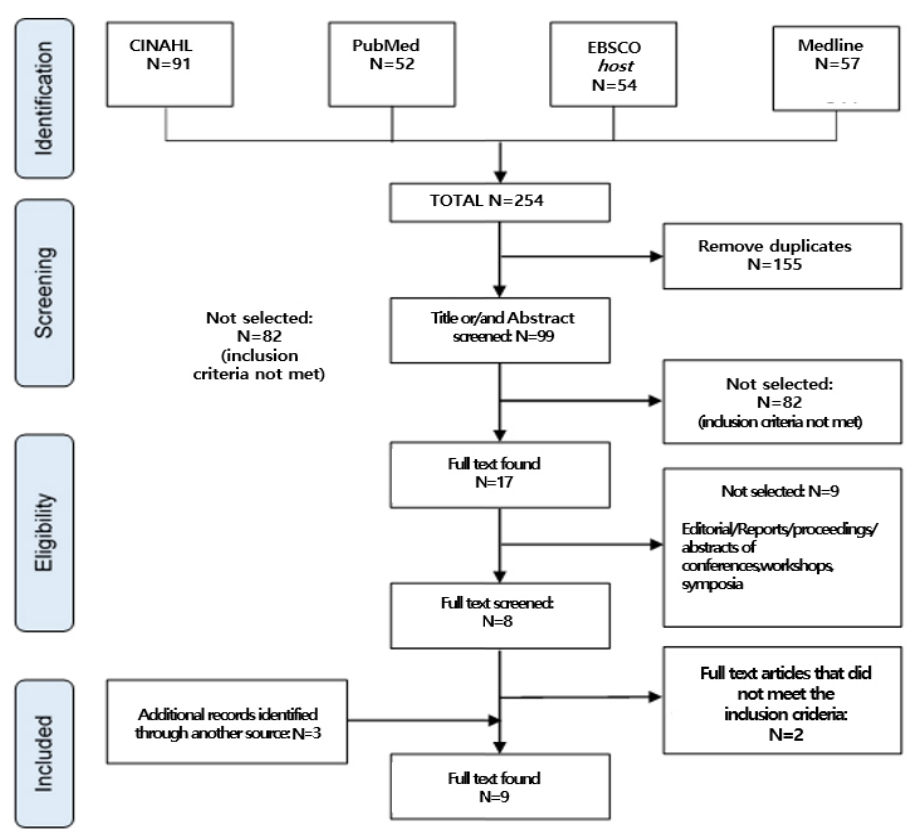
Systematic literature review was conducted following the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA). The first screening stage included deleting duplicate literature. The second stage entailed review of all titles and abstracts. Two researchers independently screened the full-text of all papers using the inclusion criteria. After completing these processes, nine studies for the final analysis were selected. Disagreement about inclusion was solved by discussion. When no consensus could be achieved, a third researcher made the final decision (Figure 1).
4. Data Extraction
The following data from the nine included studies were extracted: author, year of publication, country, period of data collection, study design, population, delirium-assessment tool, delirium incidence (%), risk factors that reached the significance level of 95% in a multivariate analysis, and risk factor’s odds ratio (OR) with a 95% confidence interval.
5. Quality Review
To assess the quality of the nine studies, the Quality Assessment Tool developed by Van Rompaey et al. [12] was used. Researchers use this tool in studies to assess the quality of risk factors. Criteria of appraisal follows.
• The study design was evaluated in accordance with the description of the aim, the design, and the methods. The size of the sample was large enough to answer the formulated research question;
• The selection of patients was clearly formulated and sustained. A severe selection bias could not be detected;
• The delirium assessment was able to review all delirious patients. A psychiatric interview or a validated assessment tool was used to diagnose the delirious state;
• Multivariate analysis was used to minimize possible confounding factors;
• The statistical analysis made the results plausible;
• The results were clinically relevant to medical or surgical intensive-care-unit patients.
6. Analysis
In this study, it was not feasible to perform a meta-analysis of the data because of heterogeneity in study designs and populations [13]. This study’s main aim was to identify risk factors not to quantify the effect size of the relationship between risk factors and delirium incidence or onset. This is why a systematic review was conducted [14]. The extracted data was synthesized through descriptive synthesis by examining study characteristics to identify common threads based on common characteristics: author, year of publication, country, period of data collection, study design, population, delirium-assessment tool, and delirium incidence (%). These are presented each risk factor’s OR.
RESULTS
1. General Study Characteristics
A total of 254 titles and abstracts were reviewed for eligibility, from which 17 original English articles were retrieved. Of these, nine fulfilled the eligibility criteria (Figure 1) including three retrospective record analyses [4,5,9], three prospective study [6,15,16], and three longitudinal studies [17-19]. No randomized clinical trials concerning risk factors on nursing homes were retrieved. Table 1 provides a detailed summary of included studies. All papers were published between 2004 and 2019. The reported incidence for nursing home delirium ranged from 3.4% to 70.3%. The lowest number of residents included was 131 residents in one nursing home [6] and the largest sample included 11,745 residents in 90 nursing homes [4]. Researchers used a variety of instruments to assess delirium including the Confusion Assessment Method (CAM) [5,9,15, 16,18,19], Neelon and Champagne Confusion Scale (NEECH NA confusion scale) [18,19], Nursing Home-Confusion Assessment Method (NH-CAM) [4,17], and Diagnostic and Statistical Manual of Mental Disorders, 5th edition criteria (DSM-5) [6].
2. Study Quality
The results of the quality assessment appear in Table 2. The description of the aim, the design and the methods were evaluated. All nine papers met this standard. In six papers, the selection of residents was clearly formulated and sustained and a severe selection bias could not be detected. The delirium assessment was able to retrieve all delirious residents. A validated assessment tool was used to diagnose the delirious state in all papers. Multivariate analysis was used to minimize possible confounding factors in all papers and the statistical analysis made the results plausible in all papers. The results were clinically relevant to nursing home residents in all papers.
3. Risk Factors
The reviewed results showed that 15 risk factors were significant in multivariate analysis in a total of nine publications. The OR of the risk factors was presented with a 95% confidence interval (Table 3). Nine factors were classified as predisposing risk factors that are resident characteristics and are often unmodifiable. Six factors were classified as precipitating factors, preceding the development of delirium, and are potentially modifiable [20].
1) Predisposing risk factors
The reported predisposing risk factors include gender, age, dementia, depression, scores on the Cognitive Performance Scale, Parkinson’s disease, hearing impairment, intravenous catheter use during the previous 24 hours, and widowhood. Researchers examined older age as a risk factor in two (22.2%) of the studies reviewed [6,9]. No association emerged between older age and delirium in five studies [4,5,15-17]. One study assessed cognitive impairment (11.1%) [4], measuring this factor using the standardized Cognitive Performance Scale. Researchers assessed dementia as a risk factor for delirium in the largest number (44.4%) of studies [5,9,16,17]. Two studies examined depression (22.2%) [4,16]. One study assessed hearing impairment (11.1%) [6]. Researchers assessed visual and hearing impairment jointly in the study [6] but found that visual impairment did not align with delirium. Intravenous catheter during the previous 24 hours scored the highest OR [6]. Researchers also found Parkinson’s disease, a chronic disease, to be a risk factor for delirium [17]. One reviewed study assessed gender (female) as a risk factor (11.1%) [15] and one study assessed widowhood as a risk factor (11.1%)[6].
2) Precipitating risk factors
The precipitating risk factors reported were pain, antipsychotics, new drugs, restraints, protein, and blood urea nitrogen to creatinine ratio. One reviewed study assessed the use of antipsychotics (used over the 7 days prior to the assessment) as a risk factor (11.1%) [5]. One study assessed an increased blood urea nitrogen to creatinine ratio of greater than 21:1 as a risk factor (11.1%) [18]. The less new drugs were used, the less likely residents were to have delirium [4]. The presence of pain aligned with delirium in one study (11.1%) [5]. Restraints were significant in two publications [6,17]. Protein (serum albumin) level aligned with delirium in one (11.1%) of the studies reviewed [19].
DISCUSSION
This is the first systematic review of risk factors of delirium in nursing home. Nine research papers were selected to perform a systematic review resulting in the identification of 15 risk factors. Only four of the 15 risk factors were mentioned more than twice. Four risk factors are age, dementia, depression, and restraints.
The incidence of delirium in studies ranged from 3.4% to 70.3%. Study patients were of different nationalities and clinical conditions, but delirium in nursing homes was a serious problem. Delirium has three motor subtypes: hyperactive, hypoactive, and mixed-motor subtype [2]. In a prior study conducted in another setting (intensive care unit, ward)[20], no studies on nursing homes were conducted that classified the occurrence of delirium. In future studies, it is necessary to investigate the classification of delirium.
In this review, four factors mentioned more than once as risk factor of delirium in the nursing home, as well as other factors that can be modified by the intervention of nurses, such as antipsychotics and pain were discussed. The risk factors for delirium are divided into predisposing factors and precipitating factors. Predisposing factors are affecting patients' vulnerability for developing delirium during hospitalization and these are often unmodifiable. These are age-related changes or patient characteristics [20]. In this review, age was an important factor in almost all papers as a possible risk factor [4-6,9,15-17]. However, age was a significant delirium risk factor in only two studies [6,9]. Age is a major risk factor for delirium in an intensive care unit [21]. However, after this systematic review, questions emerged about whether it is also a major risk factor for nursing home residents.
Dementia is the strongest predisposing factor for delirium in previous studies [22]. A study comparing the delirium incidence in dementia and nondementia groups found an incidence about two times larger among dementia groups than nondementia groups [5]. Also, in a study of dementia patients only, the highest incidence of delirium appeared to indicate that dementia is a risk factor associated with delirium [9]. However, because the symptoms of dementia and delirium are similar, delirium is often mistaken for dementia [23], causing the early detection of delirium to be missed.
In this review, depression was a risk factor for delirium. Symptoms of depression are similar to those of hypoactive delirium [24]. Symptoms of inactivity and drowsiness dominate hypoactive delirium; thus, hypoactive delirium is often misdiagnosed and overlooked [24]. People with depression may be diagnosed as having hypoactive delirium [25].
Precipitating factors are potentially modifiable and contribute to the development of delirium [20]. Use of physical restraint (chair restraints, bed rails restraints, trunk restraints) is a major precipitating factor related to delirium among nursing home residents [6,17]. The prevalence of restraint use in nursing homes is 41.0~64.0% [26]. Compared to acute setting, nursing homes have a high rate of use of restraints because they have a large number of dementia residents. Restraint use is a method to control residents' challenging behavior. Restraints are applied to protect residents and staff [26]. However staff have to be conscious of these consequences such as delirium and should consider them in deciding on restraint use.
In addition, antipsychotics are one of the precipitating factors of delirium. Older people admitted to nursing homes may have mental illnesses; medical personnel prescribe many antipsychotics [27]. Antipsychotics affect cholinergic and dopaminergic pathways and predispose elderly patients to delirium [28]. Also, polypharmacy is a risk factor for delirium [29]. Regular medication review is required.
Researchers reported pain as a risk factor for delirium in a study in several settings [30]. Pain is highly prevalent among nursing home residents [31]. Pain monitoring and treatment are important to decrease delirium of residents in nursing homes. Nursing home staff need to check residents’ pain and the interaction of residents’ medications because the use of analgesics along with antipsychotics increases the incidence of delirium [5]. The use of restraints is not only a risk factor of delirium, but also a factor that aggravates delirium [3]. This factor is modifiable and can be considered an indicator of quality of care.
Many residents in nursing homes were diagnosed with dementia and depression. The symptoms of dementia, depression, and delirium are similar, making it difficult to distinguish the delirium. This is a factor that makes it difficult for residents in nursing homes to detect the delirium, and this is the reason why the reported delirium rate is lower than the actual occurrence rate in nursing homes. In addition, the nursing home has a limited number of registered nurses who can detect the delirium. This also makes it difficult to discern the delirium. Nevertheless, most of the delirium studies have been conducted on patients in intensive care unit or post operations, rather than residents who have been admitted to nursing homes. It is necessary to conduct a study on residents who are admitted to nursing homes. Also, based on this, a delirium guideline needs to be developed.
In the many studies analyzed in this review, researchers used the Resident Assessment Instrument-Minimum Data Set (RAI-MDS) to obtain resident information [4,5,16,17]. The RAI-MDS is a standardized assessment of nursing home resident characteristics, such as sociodemographic characteristics, clinical characteristics, physical and mental status, medical diagnosis, health problems, and medication use [32]. Canadian nursing home staff use the RAI-MDS to assess all residents at admission and every 3 months thereafter until death or discharge [33]. Outside of Canada, medical staff assess residents’ health systematically, through the RAI-MDS. In the many studies analyzed in this review, risk factors for delirium were investigated using the RAI-MDS [4,5,16,17].
Although researchers assessed the relationship between various characteristics of residents in nursing homes and the incidence of delirium, no investigation was conducted on the association between the occurrence of delirium and environmental variables (such as noise or sleep deprivation). Research is needed on the relationship between environmental variables and the incidence of delirium in nursing homes. Also, although many studies described the association between staffing and quality of care in nursing homes [33], delirium was not included in quality-of-care indicators. Future studies need to assess the relationship between variables, such as the level of staffing and the level of training of personnel and the incidence of delirium.
Most of the workforce in Korea’s nursing homes are less well trained, including certified nursing assistants and care workers. The role of nurses, the only medical caregiver in nursing homes, is paramount, because nurses are the first staff to recognize changes in mental status and physical change that mark the onset of delirium. Nursing home nurses’ preventive efforts could become more focused with more comprehensive information about risk factors. On admission to a nursing home, residents with common risk factors may need to be evaluated further. Assessing risk factors for delirium may help in preventing delirium. The goal for nursing home nurses providing care is to eliminate the potential precipitating factors in each resident’s condition, and to provide supportive interventions that address residents’ predisposing factors.
CONCLUSION
Fifteen risk factors, six precipitating and nine predisposing, influence the onset of delirium in the nursing home. These can be used to develop a checklist of risk factors for nursing home delirium. Use of such a checklist may facilitate the ability to identify residents with a high risk of developing delirium and detect delirium at an early stage and thereby provide a suitable treatment when indicated. These types of management might decrease the negative consequences caused by delirium after dwelling in a nursing home. Further studies should investigate whether improving modifiable risk factors actually leads to a decreased incidence of nursing home delirium. Also, additional risk factors should be assessed in nursing homes, including environmental variables and nurse-staffing factors.