Preparing for the Trend of Aging in Place: Identifying Interprofessional Competencies for Integrated Care Professionals
Article information

Abstract
Purpose
The purpose of this study was to identify interprofessional competencies for the integrated community care of older people.
Methods
This study used a methodological approach, and the specific process aimed to identify the components of interprofessional competencies for integrated community care using a scoping review and validating the identified competencies with the Delphi method. The scoping review first identified relevant studies through the following electronic databases: PubMed, CINAHL, Embase, and the Cochrane Library. We then selected studies that met the inclusion criteria and analyzed their results to identify a draft version of the competencies. Expert panels validated the list of competencies through two rounds of the Delphi survey.
Results
The two rounds of the Delphi survey revealed consensus. Finally, we developed an interprofessional competency for integrated community care comprising 19 interprofessional core competencies, 20 integrated core care competencies for community care administrators, 13 integrated core care competencies for care coordinators, 13 integrated core care competencies for local service providers, and 12 integrated core care competencies for community health leaders.
Conclusion
This study can help inform job descriptions, evaluate the relevant professionals’ performance, and develop a competency-based curriculum for better practice.
INTRODUCTION
The world’s population is aging rapidly [1]. It is expected that older people could account for 12 percent of the global population in 2030 and 16 percent in 2050 [2]. Most countries are confronted by the challenge of caring for the increasing number of older people, especially because of the increasing demand for care services to address multiple chronic conditions common in older age and the increasing need among older people for assistance with daily activities such as dressing, bathing, and preparing food [3]. However, the majority of older people want to stay at home as long as possible [4]. ‘Aging in place’ is defined as people who are living in the community with some degree of independence, rather than being admitted to a residential care facility [5]. To successfully realize ‘aging in place,’ it is essential for health-care professionals to focus on individual needs, housing environment, and adequate community-based services that support health and well-being [6].
Despite the increasing numbers of people with complex health and social care needs, healthcare delivery has traditionally focused on caring for illness, rather than caring for the people themselves [7]. To cope with older people’s individual complex care needs, integrated healthand social-care services are considered crucial [8,9], and when health and social care professionals collaborate in this endeavor, integrated person-centered care becomes achievable [10]. How then, can we facilitate such collaboration? Caregivers are required to be skilled in working with other professionals [11] as well as appropriately meeting the comprehensive needs of older people [12]. Such interprofessional competencies for the integrated care of older people may help address their burgeoning needs by providing quality services.
Previous attempts to identify integrated care competencies for caregivers of older people have been restricted to the generic competency components of interprofessional care, or have focused mainly on the aspects of care coordination of integrated care [13,14]. However, as integrated care is provided at multiple levels such as at the system, service, and personal levels [15], professionals who work at each level may take on distinctive roles. Thus, interprofessional competencies for the integrated care of older people should be more specifically defined based on the roles of relevant core professionals to promote quality care for older people.
The purpose of this study is to identify interprofessional competencies for professionals who provide integrated community care for older people. The specific aims of this study are:
• To identify the initial components of interprofessional competencies for the integrated community care of older people
• To validate the identified interprofessional competencies
METHODS
1. Design
This study is a methodological research to identify interprofessional competencies for the integrated community care for older people.
2. Phase and Strategy
The study includes two phases of work. In the first phase, a scoping review [16] is used to identify the initial components of interprofessional competencies from current international sources. In the second phase, the paper uses the modified Delphi method [17] to validate the competencies from expert consensus. The method uses a chain of rounds and starts with a questionnaire or an interview to solicit the recruited experts’ opinion and comments related to aspects of the study’s investigation [17]. Finally, the interprofessional competencies are identified (Figure 1).
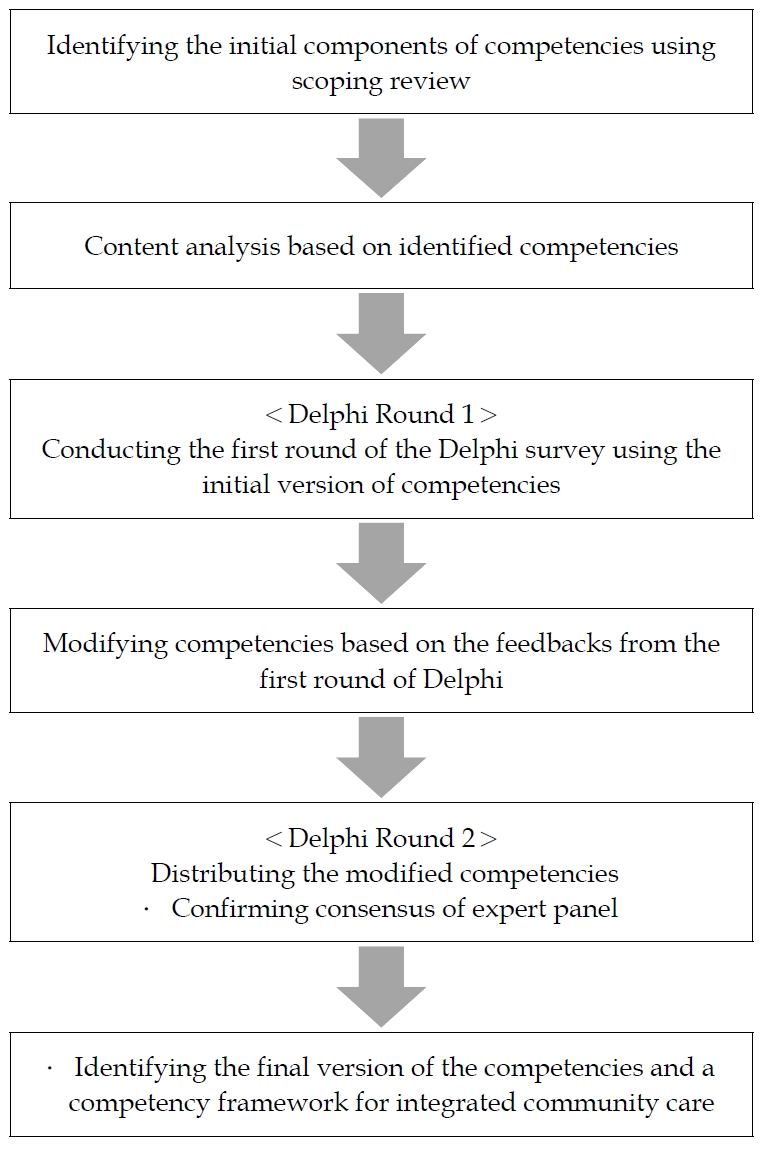
The phase and strategy of this study.
1) Phase 1. Generating the initial version of interprofessional competencies
(1) Search strategies
Journal articles, books, and reports based on the inclusion criteria were collected from four databases: PubMed, CINAHL, Embase, and Cochrane Library. The keywords search strategy was employed using all terminological variants of (“integrated care” OR “collaborative care” OR “health and social care” OR “interprofessional care” OR “interdisciplinary care” OR “multidisciplinary care” OR “multiprofessional care”) OR “Delivery of Health Care, Integrated” complying with MeSH (Medical Subject Headings) terms AND “Competence”.
① Eligibility criteria
The study included reviews of journal articles, reports, and grey literature published from 1990 through 2020. This review did not define the evidence of certain interventions, so the study design and quality were not limited. Literature written in Korean and English was included.
② Inclusion criteria
• The competencies described are scoped mainly to the workforce
• The competencies that are defined, referred, evaluated, or compared relate to integrated care
• The workforce that is referred to is relevant to health and social care in the community
③ Exclusion criteria
• Competencies that referred only to caring for specific patient groups or focused on a clinical care setting were not considered for this review
After removing duplicate studies, we selected studies based on titles and abstracts and finally, reviewed full text studies that met the inclusion criteria.
(2) Data extraction and synthesis
If the literature met the inclusion criteria, data relevant to interprofessional competencies for the integrated community care of older people were extracted. The extracted data from the reviewed literature were included in data extraction records and synthesized in data-summary charting form. Key information, such as authorship, article type, country, and list of competencies were included in Table 1. Then, the information organized in charting form was collated and reported from the literature’s descriptions of interprofessional competencies for the integrated community care of older people. The competencies were finally analyzed using content analysis [27] Two researchers independently analyzed the competencies to identify different concepts and categorized the contents. Then, the two researchers compared all the categorized competencies and made changes. They verified the contents and wording of the competencies to reach consensus. Finally, the drafted version of competencies was identified.
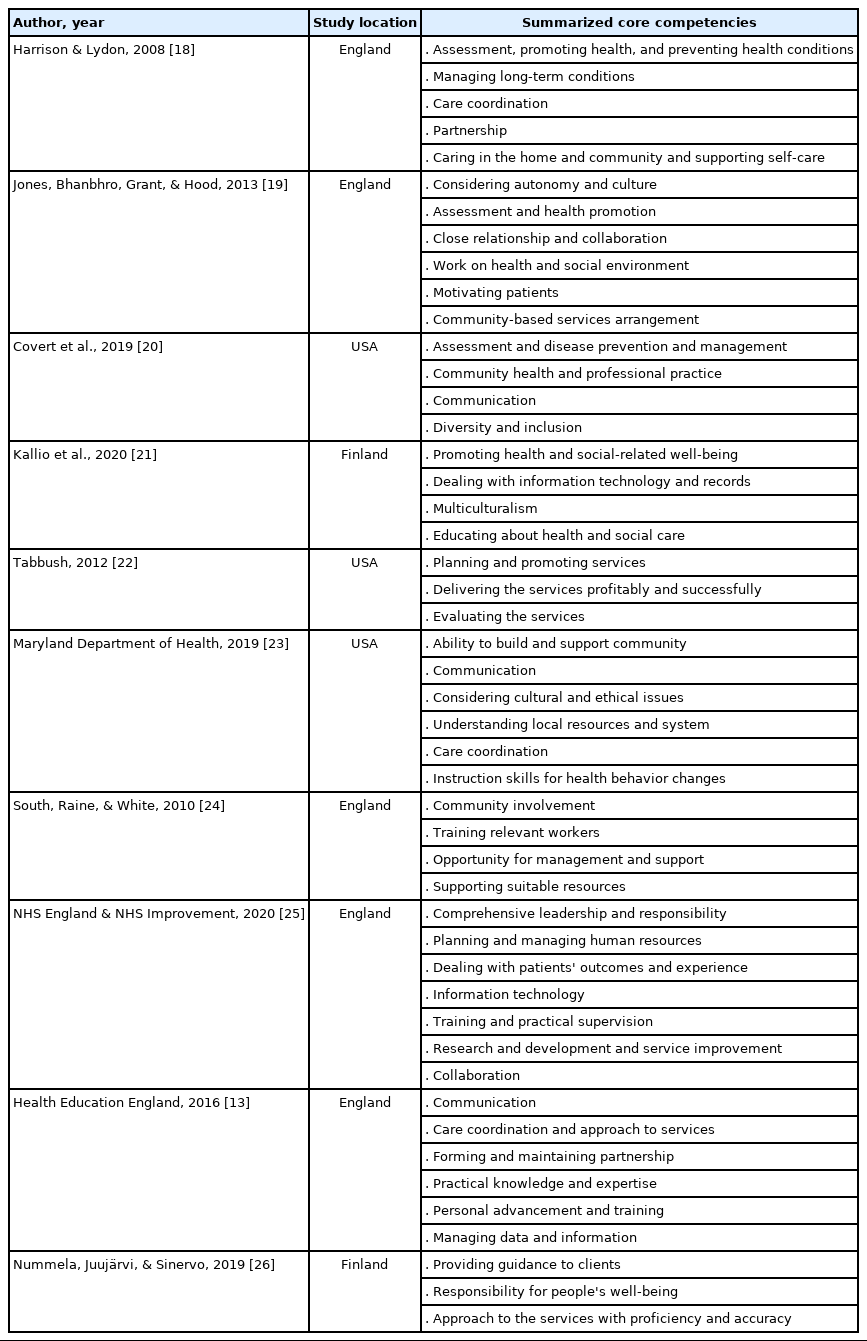
Literatures Identified in the Scoping Review
2) Phase 2. Experts identify the validity of the competencies
(1) Expert group
For the two rounds of the Delphi survey, experts were recruited from the health and social care fields to form an expert panel. The panel included professors or professionals experienced in researching the field of caring for older people, or who had delivered care to older people within the community. Purposive sampling was used to recruit participants for the study. To produce a comprehensive list of experts, conference proceedings and articles published in the journal related to health and social care were reviewed to identify the authors, and the organizations and institutes related to health care and social services in the community were asked to recommend appropriate experts. The professors and researchers were selected based on their strong records of publications and presentations related to integrated care for older people in the community. The selected practitioners were working in institutes providing health care and social services in the community and had at least 3 years of working experience. An email invitation was sent to each candidate of expert panel. Finally, ten experts participated in the Delphi survey (Table 2) (Delphi typically recommends the participation of ten to 15 participants) [28].

The Characteristics of Expert Panel
(2) Procedures and analysis
The purpose of the Delphi was to reach consensus on each component of the core and job-specific interprofessional competencies for the integrated community care of older people. To establish validity, researchers and professionals with research or working experience in the area of integrated care in the community conducted a pilot test to review the initial list of competencies and complete the Delphi survey. After the pilot test, minor revisions were made to the statements in the questionnaire to facilitate the potential respondents’ understanding of the meaning of the sentences. The final version of the questionnaire was distributed and collected by e-mail. The responses to the questionnaire in each round remained anonymous to inspire the participants to actively rate the questionnaire. The questionnaires were given to the participants at two time points and were subsequently collected. In each round, the participants were given two weeks to complete the questionnaire. The second questionnaire was drawn up based on the reviewed data from the previous round.
3. Round 1
A survey questionnaire was distributed to all participants, and their responses were rated on a 5-point Likert-type scale ranging from 1 (strongly disagree) to 5 (strongly agree). The questions related to each component of the interprofessional competencies required for the integrated community care of older people. All participants were also asked to explain their rating and to recommend new components of competencies if they felt the need to do so.
4. Round 2
Based on the experts’ opinions, statements of competencies that were incongruent with the aim of the study or perceived to be duplicates were deleted before Round 2 was conducted. A brief summary of the modifications made based on the experts’ comments and the questionnaire, including the revised components of competencies, were then distributed to the expert panel. The feedback from Round 1 was presented as the mean and SD scores of all the experts on the panel. The participants were given the initially checked score of each statement and asked to reconsider their initial decisions about ambiguous statements made from Round 1 and express their agreement with the new statements.
After completing all rounds of the Delphi, the data were analyzed with SPSS (Statistical Package for the Social Scientists) software version 22.0 for Windows (IBM Corp., New York, NY, USA). The content validity index (CVI) was used to calculate content validity [29]. This study used the content validity index for items (I-CVI), and the overall scale (S-CVI) to calculate the S-CVI/Ave. It followed the standards recommended by Lynn (1986) [29] (with six to 10 experts, the minimum score of I-CVI =.78, and the S-CVI/Ave=.90 or higher).
5. Ethical Consideration
This study was approved by the institutional review board of Chungnam National University (Approval no. 202009-SB-121-01).
RESULTS
1. Generating the Initial Competencies
The primary search returned 95 documents, 10 of which met the inclusion criteria and were reviewed (Figure 2). Five were British-based documents, three were USA based, and two were Finland based. After conducting content analysis of the interprofessional competencies relating specifically to the care of older people extracted from 10 records, 77 subcategories were identified and became a set of competencies. The 77 subcategories were grouped into five categories based on each professional’s role and work within integrated care (Figure 3).
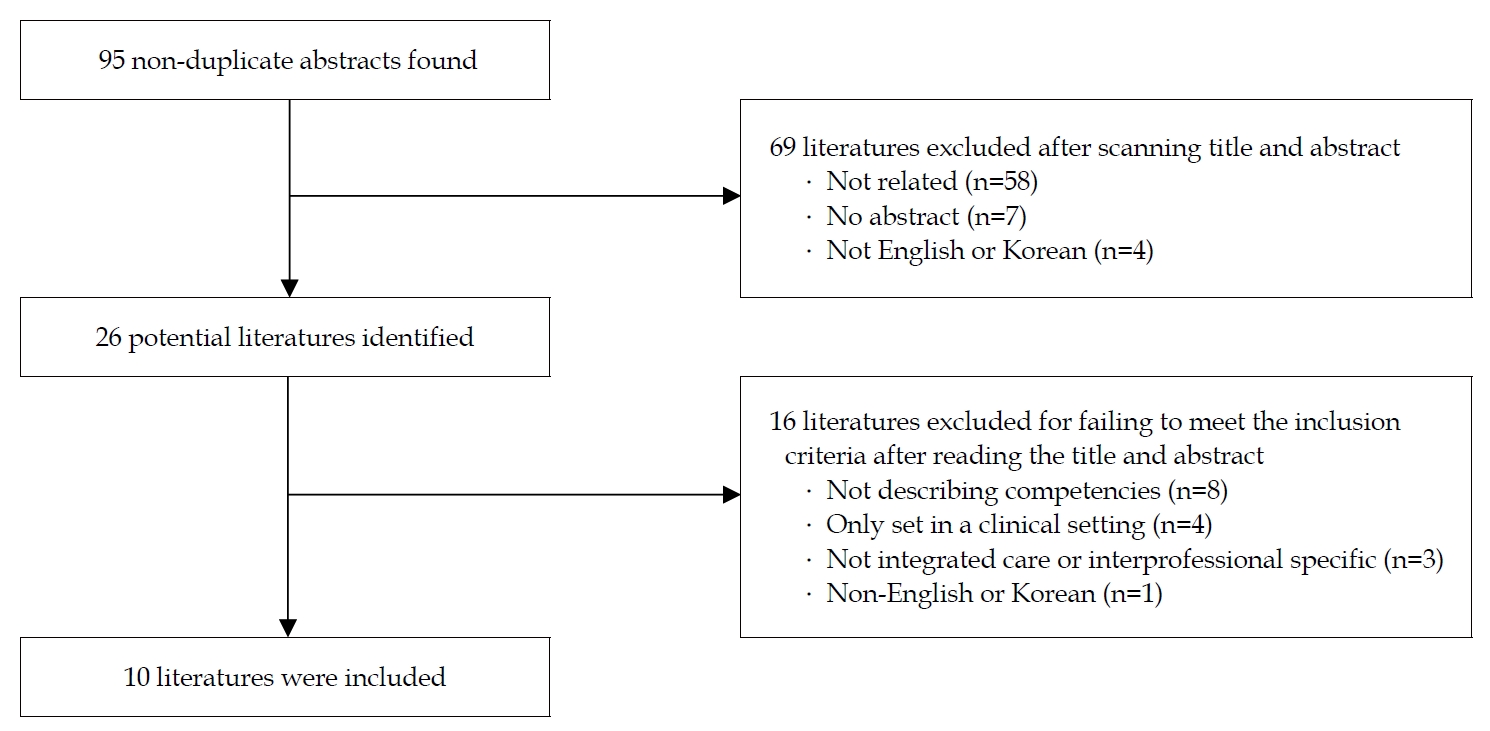
Process of document selection in scoping review.
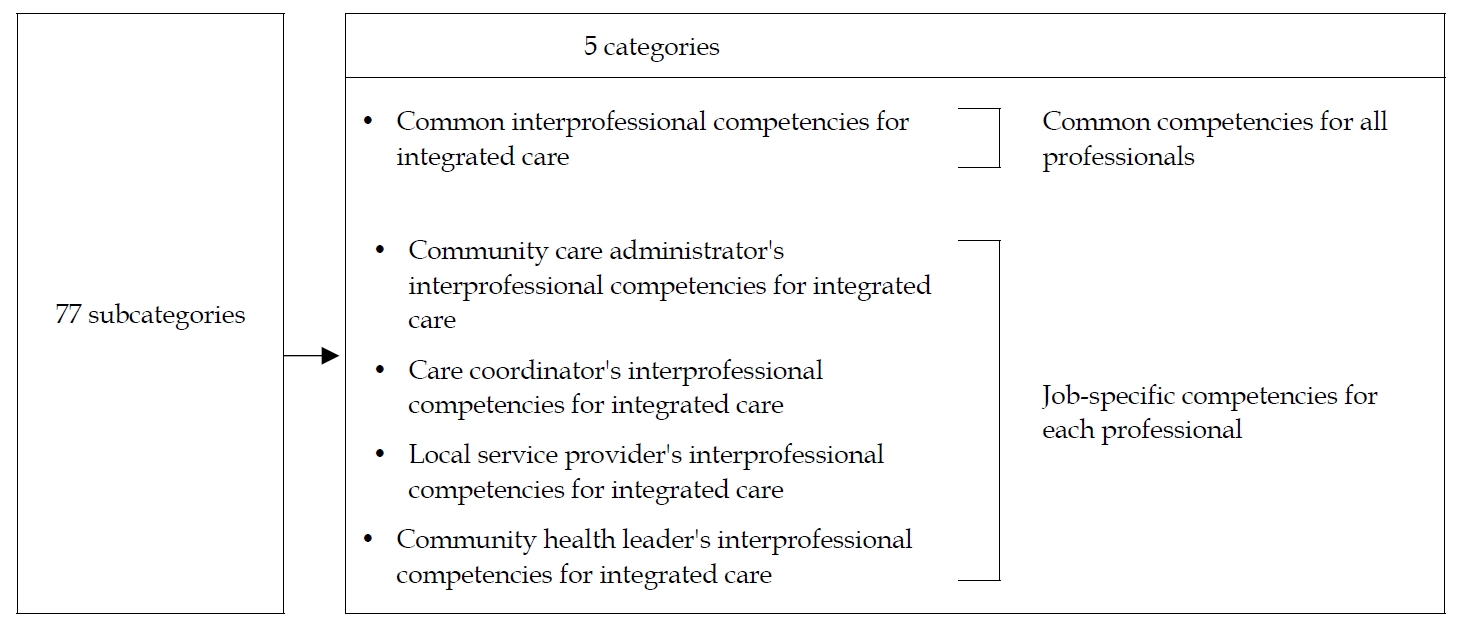
The results of content analysis based on the scoping review.
2. Establishing Validity through Expert Consensus
A total of ten experts completed the Delphi survey, and after two rounds, consensus was reached on the components of the competencies. The survey was conducted anonymously; anyone who participated in the survey could not be distinguished from the other participants to ensure reliability of the responses.
In the first round, the expert panel reached a consensus level of 0.8 for 19 out of 21 interprofessional core competencies for the integrated care of older people; the two competencies on which there was not consensus were deleted. The panel did not suggest any new competencies, but minor revisions were made to four competencies based on the expert panel’s recommendations. Of the initial 20 integrated care core competencies for community care administrators, 18 items reached the consensus level, and two competencies on which the experts did not reach consensus were deleted. The panel revised one competency and proposed one new competency: planning finance, budgeting and business, and monitoring the cost-effectiveness of the use of finance and resources. Of the initial 12 integrated care core competencies for care coordinators, all competencies reached the consensus level. The expert panel suggested one new competency: improving the work process based on integrated care performance results. Of the 18 initial integrated care core competencies for local service providers, 11 competencies reached the consensus level and seven competencies were deleted. The expert panel suggested two new competencies: sharing resources and information with relevant organizations to benefit community residents and helping community residents confront emergency situations/crises. Of the 11 initial integrated care core competencies for community health leaders, all competencies reached the consensus level. One additional competency was suggested and modification of some competencies was suggested before Round 2.
In the second round, a high level of support was attained for all modified and additional competencies (The I-CVI for interprofessional competencies for the integrated community care of older people ranged from 0.9 to 1.0, and the S-CVI/Ave was 1.0). Therefore, consensus on all interprofessional competencies was reached.
Five parts of interprofessional competencies for the integrated community care of older people, including the 77 competencies, were identified (Table 3). The first part presents the common interprofessional competencies for the integrated community care of older people, which are 19 common competencies for all integrated care professionals. The last four parts present the interprofessional competencies for each professional relevant to the care for older people in the community: 20 competencies for community care administrators, 13 competencies for care coordinators, 13 competencies for local service providers, and 12 competencies for community health leaders. Finally, based on the identified competencies, a set of interprofessional competencies was identified for integrated community care (Table 4).
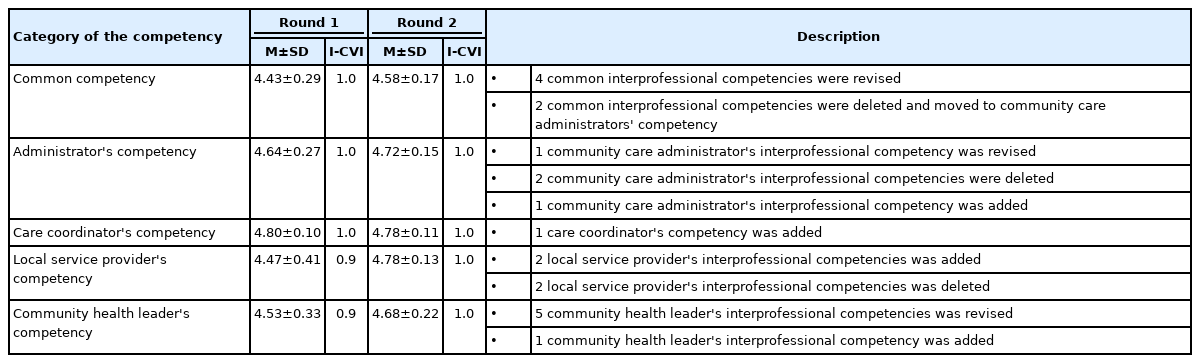
The Result of Delphi
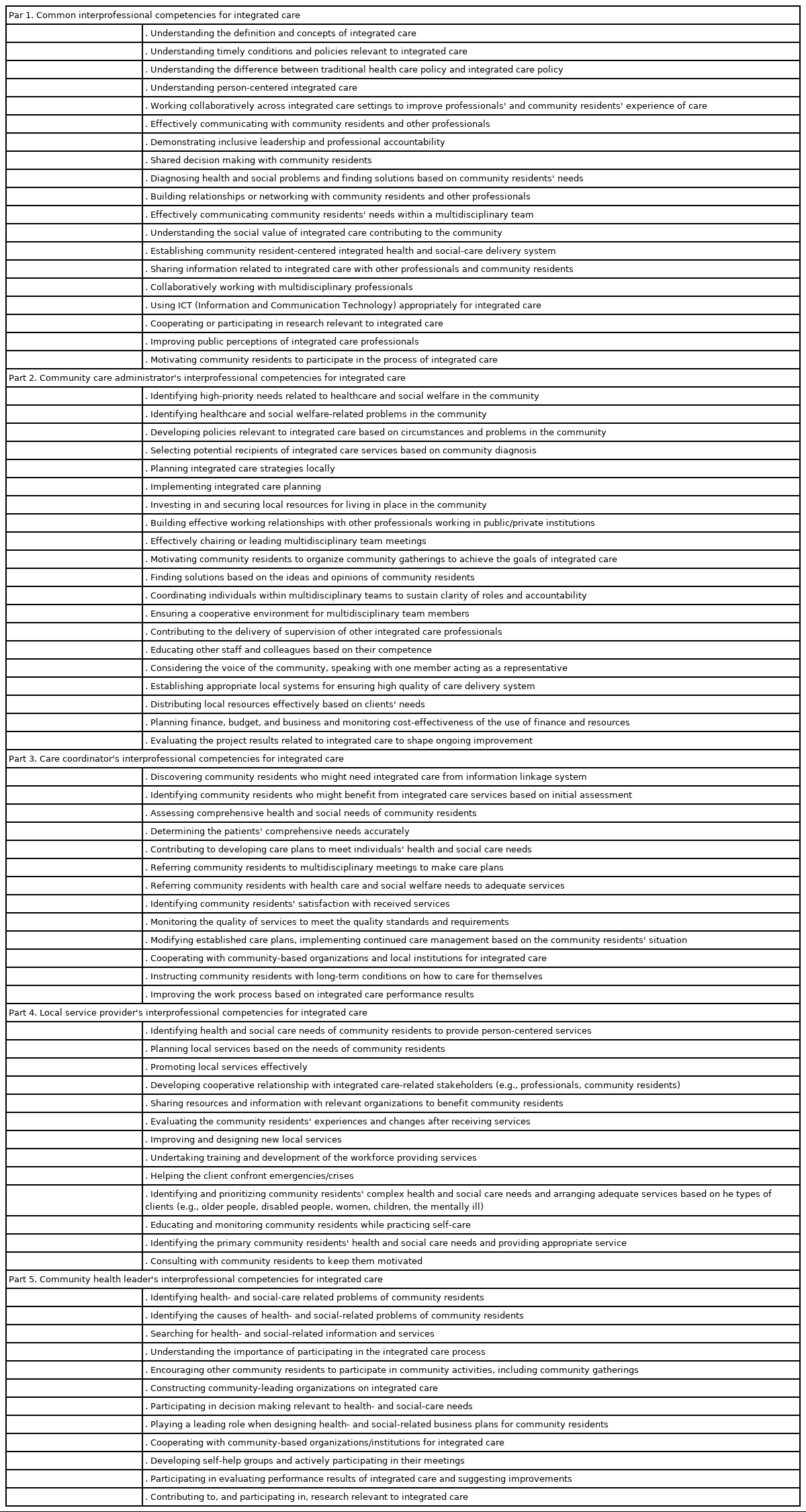
The Interprofessional Competencies for Integrated Community Care
DISCUSSION
This study aimed to extract a set of interprofessional competencies for the integrated community care of older people based on the results of a scoping review and validation through a Delphi survey. Seventy-seven competencies across five parts were identified to promote an integrated approach to the care for older people. This was the first attempt to provide a set of interprofessional competencies for the integrated community care for older people, which includes both the common and job-specific competencies of integrated care professionals and extends the range of included professionals (a local health provider and community health leader, who played a leading role). In addition, the identification of interprofessional competencies for integrated care can serve as the basis for much future work on competency-based practice. For example, the competency framework can serve as a guide to how the defined competencies can be applied in different work settings and help identify the roles of each professional [29]. This competency framework can be useful for standardizing terminology to explain a range of practices and design relevant training [20].
Previous studies identifying interprofessional competency frameworks have often described the general components of interprofessional care, such as teamwork, leadership, and communication skills [14,31]. However, to present a clear direction for professionals, more specific competencies that can lead to appropriate action for older people are required. In addition, previously identified competencies relevant to integrated care in the community have often focused on the characteristics of care coordination [13,20,25]. Specific collaboration among professionals in health and social care is important to ensure optimally integrated care practice [32] and that integrated care is implemented at the system, service, and personal levels [15]. This indicates that integrated care professionals would be required to collaborate in multiple situations and work at different levels. In this respect, their competencies need to be specifically defined and they must be able to apply these competencies in their work. Therefore, to design the competency framework, the jobspecific competencies of each professional were considered, except for overlapping components shared by all professionals. Each component of competencies was described in as much detail as possible.
The common component of competencies all professionals needed was the fundamental knowledge and skills required for better collaboration, such as interprofessional practice, the nature of integrated care and communication, and teamwork. This result is mostly consistent with the results reported in previous studies [20,31]. Those competencies are relatively general and essential components for all professionals to work interprofessionally among older people. The competencies include key elements for collaboration. When crafting a fundamental training course for all integrated care professionals, these competencies could be considered as evidence.
The identified integrated care core competencies for community care administrators were: establishing policies, improving the community environment, reflecting the health and social care needs of the community, and supporting the general process of integrated care practice. This result aligns well with the characteristics of the system- level implementation of integrated care, which focuses mainly on strengthening system governance and accountability systems [15]. One previous study also reported that administrators support interprofessional practice, and that they consider the strategies, structures, and cultures related to their interprofessional works [33]. The findings indicate that identifying integrated care core competencies for community care administrators would contribute to constructing an administrative foundation for integrated care, considering the relevant workforce and financial management.
The identified integrated care core competencies for care coordinators focus mainly on inspiring community residents to participate in health- and social-related activities and connecting them to community-based care services [13,34]. This result is similar to the competencies identified in previous studies. The core competencies of ‘care navigators’ are to support individuals’ ability to conduct health-promoting activities [35] and establish increasing partnership between a person and a relevant provider [36]. ‘Link workers’ are also competent for assessing comprehensive care needs and connecting people to accessible services [34]. This finding presents that to effectively develop care workers’ competencies, a practicum- based curriculum would be significant because these competencies are required to be continuously interactive with clients in practice.
The identified integrated care core competencies for local service providers are: developing new and quality health- and social-care services and delivering local services based on clients’ complex needs. Community-based organizations are required to possess leadership and management skills [22] as well as provide appropriate direct health- and social-care services (e.g., rehabilitative exercises, nutrition consultation, chronic disease management) [37,38]. The findings indicate that when developing local service providers’ integrated care core competencies, training needs to focus on strategies that identify the comprehensive unmet needs of individuals and improve service quality and the delivery process, based on the clients’ satisfaction.
The identified integrated care core competencies for community health leaders focus mainly on leaders playing a meaningful role as proactive members of the community by being involved in decision-making relevant to the integrated care system and encouraging other resident peers to participate in community-based health and social activities to enhance the well-being of the older people. Previous studies similarly have reported that leadership roles should include active participation in decisions related to policies that are important to their community. Such studies also concur on the suggestion that leaders and other stakeholders should proactively develop a health-promoting culture in the community and engage in local community affairs [24,39]. Person-centered integrated care needs community residents’ involvement in the process of integrated care, and these residents must be considered partners. In addition, those community members living in close proximity to other community members who need help with well-being-related issues could empower other community residents to become involved in health-promotion activities as well as helping them overcome the community’s health- and social-related problems [24,39]. Community health leaders could be both proactive participants and frontline workers who can reach their community nearby and be familiar with community members. In this aspect, community health leaders should be deemed an essential component of integrated care because it could be a significant trigger for successful community residents’ involvement in the process of integrated care. To help community health leaders seize opportunities to become equipped with the appropriate competencies, structured education training in fundamental knowledge of health and well-being should be actively promoted. This would ensure that individuals understand their roles and capitalize on interprofessional learning opportunities [40].
We propose several directions for future studies. First, the focus of this study is to identify interprofessional competencies for integrated care for relevant professionals. This study defines and presents a list of comprehensive interprofessional competencies for integrated care to help each professional become competent in their work. However, to better prepare professionals and enable them to meet the complex needs of older adults, further studies need to explore ways to develop the interprofessional competencies of relevant professionals using effective training and competency-based education programs. In addition, the factors that prevent professionals from applying their competencies in terms of upgrading policies and systems should be identified and eliminated so competent professionals can achieve comprehensive interprofessional care.
Limitations
This study was conducted in Korea to identify competencies for integrated care in the community. In order to apply this competency internationally, some statements relating to the required competencies may need minor adjustments based on the context of each country because each country has different policies, health-care delivery systems, and cultural characteristics.
CONCLUSION
The research and literature used in this study focused on identifying interprofessional competencies for an integrated care framework that incorporates health care and social services. With this knowledge and the appropriate attitude and skills, integrated care professionals will be better prepared to provide leadership in working with the complex needs of community residents and collaborate with multidisciplinary workforces. The competencies can be used to inform job descriptions, enlist planning professionals, and evaluate them to identify who can provide integrated care in a community setting in terms of applying the appropriate knowledge and skills that will lead to the enhancement of integrated care that addresses the health and social care needs of older people in the community. Such enhancement will help these older members of the community age in a place where they want to stay with independence and dignity for the rest of their lives.
Notes
The authors declared no conflict of interest.
Study conception - CEJ and PM; Design acquisition - CEJ; Data collection - CEJ and PM; Analysis and interpretation of the data - CEJ and PM; Drafting and critical revision of the manuscript - CEJ; Final approval - CEJ and PM.
Acknowledgements
This paper is based on first author's dissertation for the degree of doctor of philosophy in Nursing.